Mandibular Matrix – One Incision Jaw & Chin Implant Augmentation
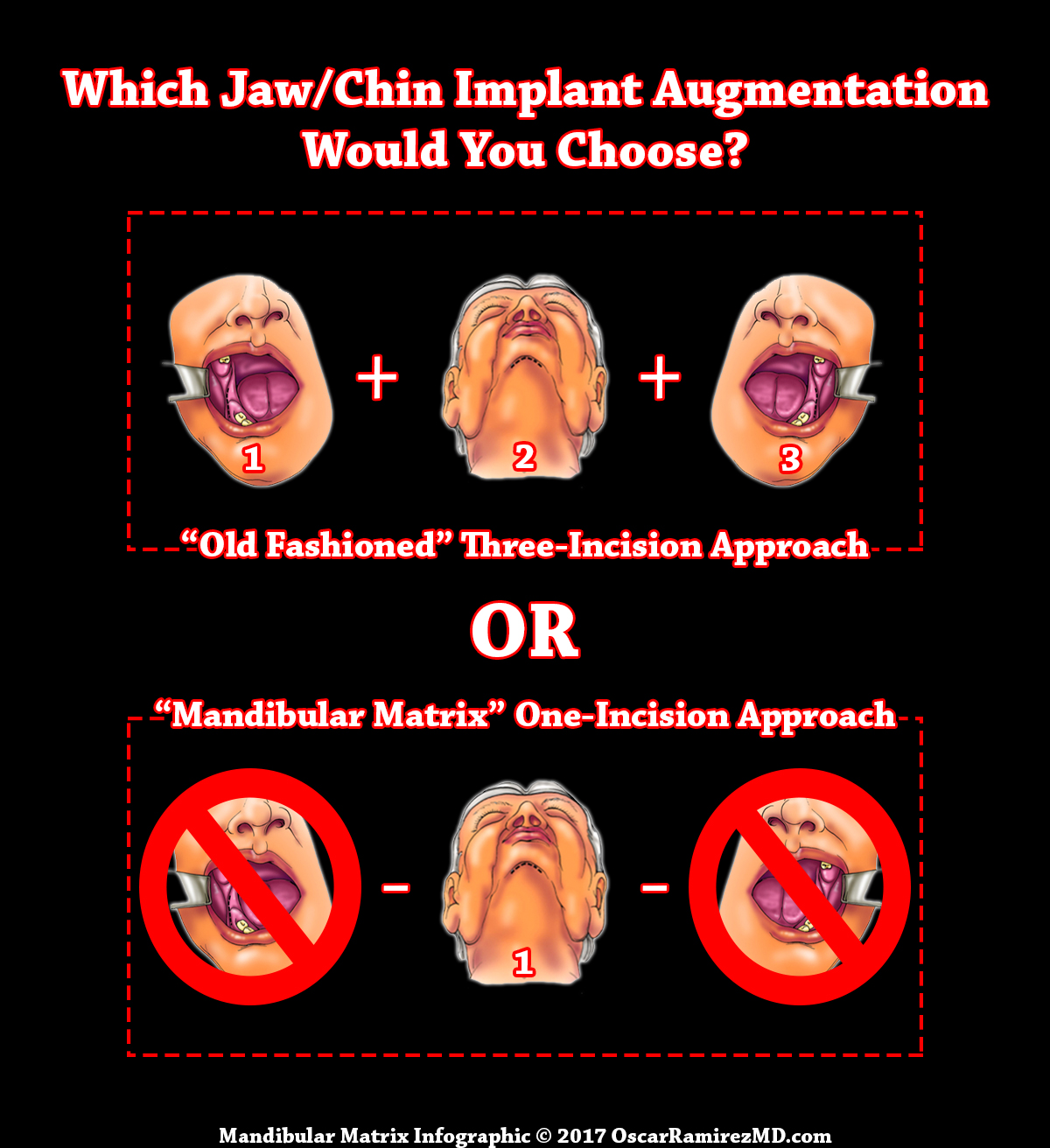
“You will find that most doctors still perform Jaw and Chin Implant Augmentation via an “Old Fashioned” Three-Incision Approach. In order to make a One-Incision Approach possible, I had to invent a Specialized Endoscopic Procedure, Custom Surgical Equipment and Wrap-Around Design Implants. These THREE COMPONENTS (Endoscopy, Surgical Equipment and Implants) allowed me to successfully switch from the Three-Incision Approach to a One-Incision Approach and the “Mandibular Matrix” was born!” -Dr. Ramirez
History
Back in the 1990’s I developed a Jaw and Chin Wraparound Implant System called, “The Mandibular Matrix”. In the years leading up to that point, I typically performed Jaw and Chin implants through a semi-open technique. This required a combination of two large incisions behind the molars inside the mouth and another incision in the sub-mental area under the chin. In some cases, patients opted for an intraoral incision, instead of the submental incision for placement of the chin implant which meant a whopping three incisions in the mouth !
The ability for me to reinvent this unique technique came about through my many years of performing other surgeries with Endoscopic Tools. It meant that I could perform this operation through a SINGLE SUB-MENTAL INCISION which is under the chin. In order to perform this, it required further development of endoscopic techniques and special instrumentation to be able to separate the soft tissues from the bone at the sub-periosteal plane. At the same time, I also invented specific implants for this procedure that would allow precise placement onto the bone. The implants are very unique in that they do not require multiple screws to secure them unlike other jaw implants that require several screws into the bone. We will discuss the Implants in more detail later on this page, but please see the following video to gain an understanding of how the entire Mandibular Matrix works:
Mandibular Matrix Video

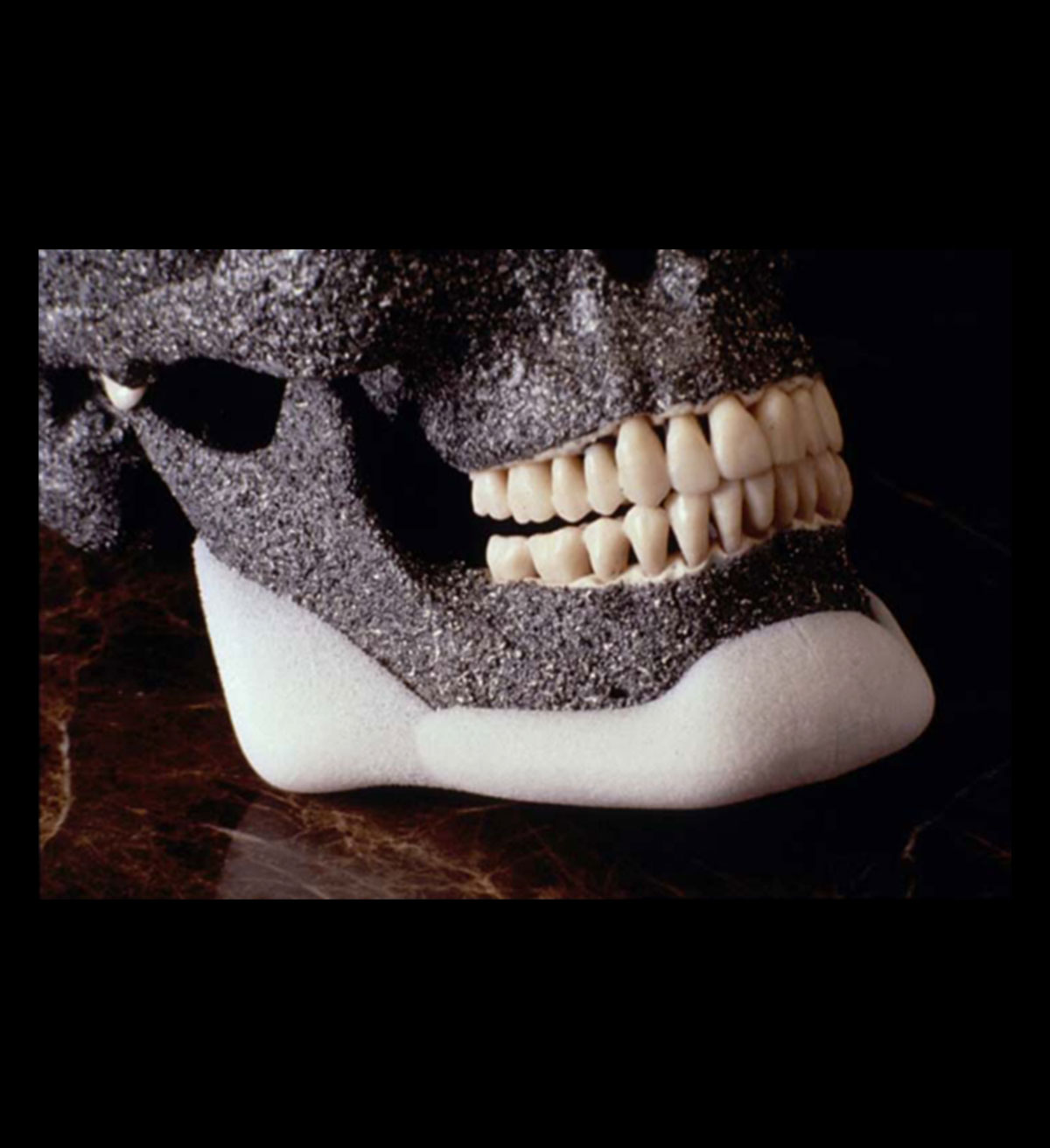
Implant Design
The implants have been designed to provide a three-dimensional ”restoration of the mandible.” The wrap-around component of the inferior border provides additional self-stabilization to the implant. Additionally this provides a vertical augmentation of the chin and mandible. This is a significant advantage compared with two-dimensional onlay type of implants made of silicon or Porex materials. Despite their rigidity the components of the system allow insertion of the implants to restore the entire mandibular contour through minimal access incisions. The MMIS is composed of a two-piece extended wrap-around chin implant and separate gonial implants (right and left) made of high-density porous polypropylene. The pre-jowl implants can replace the chin implant in some patients and also can be added to the system when necessary. The gonial angles can be combined with newer different shaped implants to accommodate different patient’s requests and esthetic needs. For the chin area I have designed a new set of implants called Mento-pagonial or button chin implant that comes in small medium and large sizes. The gonial angle implants can be combined with one of the different sizes button implants for patients that request a break between the contour of the angle of the jaw and the chin. Some patients perceive this esthetically superior to the U-shaped implants. The combination of the gonial angle with a short geniomandibular or the button chin implants give the so called V-shape jaw line versus the overlapping of the gonial angle implant with a geniomandibular implant giving more of a U-shaped jaw line.
I will recommend to you to have complete imaging and morphing by professionals that are dedicated to this endeavor. A complete facial morphing may take up to a full day of work or even more and this is not of practical use in our practice. We have a simple software for computer imaging that we can do minor morphing of the face. The office can guide to you some professionals that do this type of morphing. I will not recommend specifically one that but will leave it up to you to research their experience and expertise. However I have received a study of morphing done by those professionals and I found it useful mostly in communicating and in understanding better the realistic expectations that the patient have.
We can show you the implants and place it on top of your pictures; however this wont give you much light I in terms of the results that you may be looking for. Along those lines there is no specific software program that I know about that can input the sizes of the implant for each patient and see the response of the soft tissue in those implants and morphing. The computer imaging and software are only for communication purposes, but not as a way to predict what your specific outcome will be. For your comfort I will tell you that in about 50% of our cases our results can be even better than the computer imaging or morphing. This is probably due to the fact that professional morphers make changes that are more conservative with the possible surgical outcomes.
- The whole matrix system with chin implants and gonial implants.
- Midface lift?
- Buccal fat pad mobilization?
- Cervicoplasty anterior approach with suture suspension?
- Fat excisions of the neck?
You can have part or all of the surgery that you have mentioned. However, the indications for each one of the procedures need to be determined after seeing your pictures and after face-to-face consultation. If your question is more specific and you ask me: can you do all of these procedures at once? The answer is yes, it can be done, and however this will take a whole day’s work, which is about eight hours. In some cases if there are some difficulties with your patients or your patients are too heavy that the surgery might be even prolonged. If that is the case we may need to split the surgeries in two stages.
Although some patients feel the sensation of tightness of the neck this is temporarily mostly related to the tightness of the soft tissues rather than the suture suspension itself. I have never seen any patient with breathing problem related to this.
The standard or simple x-rays are not useful to study asymmetries of the face. Plane x-rays are good for patients who have had silicone implants to see if there has been any bone erosion. To study the asymmetry of the facial skeleton the best option is to obtain tridimensional CAT scan. Even better is to obtain an acrylic facial model construct based on the tridimensional CAT scan. This has been described at length in the section of facial matrix and custom-made implants.
The gonial angle implant and the chin implant are introduced through the same incision underneath the chin. As I mentioned in the section of surgical techniques and complications I prefer the submental incision to the intraoral incision because the incidents of infections is higher with the intraoral incisions.
As it was described before exactly the opposite happens. The silicon implant has higher rate of bone erosion and migration.
The implant is hard and less brittle to blunt injuries than the chin or mandibular bone. If you receive forces applied to your jaw that is enough to break your bone it will probably break your bone rather than break the implant. It is feasible that the extra support provided by the implant might be a protective factor for the development of a fracture of the mandible although this has not been proven scientifically.
The gonial implant is up to 11 mm in projection. This projection is around the tip of the implant mostly. The lateral or inferior projection can be carved to the patient’s requirements. In other words if the patient wants more lateral augmentation the inferior border will be trimmed more or vice versa. If the patient wants vertical augmentation then the lateral projection will be trimmed.
The chin implant will be fixed with screws.
If you have an ugly or unsightly scar. This can be revised during the time that we place a mandibular matrix implant. In other words we will use the same incision after the scar removal to place the implant. However if the previous scar is too anterior on the chin we may have to place another incision in the most appropriate location, which is posterior to the submental crease. Later on the preexisting chin scar can be revised.
You will have tri-dimensional augmentation of the chin in the anterior, vertical and lateral projection. However each section of the implant can be carved to give any specific projection that you require. In other words if you need less vertical projection the vertical component is trimmed off. If you like less lateral projection the lateral extents are trimmed off etc.
The projection is given by the size of the implant and the repositioning of the soft tissues. As I mentioned in the description of the implant in relation with soft tissues the soft tissues tends to remodel better over the Medpor implant. The highest projection of the chin implant is 7 mm, however with the soft tissue remodeling and the tissue on-grow around the implant the final chin projection can be as much as 12-15 mm.
I will recommend a round one if you are going to use a larger implant. The large implant will give some squareness to the chin. However, if you really want a very defined result with significant squareness of the chin then the square implants will be used. If you do not require significant augmentation of the chin the smaller square will provide a very natural squareness of the chin.
The removal of the entire capsule of the old silicon implant can be dangerous to your soft tissues. Because of the adherence of the muscle and nerves to the capsule those structures can be in jeopardy. However when we do replace the silicon implant with a Medpor implant the posterior capsule is removed. The underlying bone is smoothed down to allow the perfect coaptation of the implant to the contour of the chin leaving the existing anterior capsule over the implant usually does not produce esthetic deformities. There is a higher chance of esthetic deformities if you try to remove the anterior capsule. If the capsule is too tight we will do some cross-hatching to the capsule to allow better accommodation for the soft tissues to the implant.